
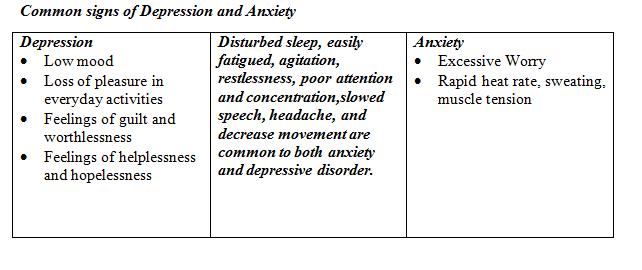
Depression and Anxiety are among the most prevalent mental disorders in our community. Patients with depression often have features of anxiety, and those with anxiety disorder commonly also have depression. Both disorders frequently occur together, meeting criteria for both.
Depressive and Anxiety Symptoms are also common among people who are suffering from other medical conditions such as cancer, traumatic injuries, cardiovascular diseases, etc. Research states that 47% cancer patients and 33-64% patients suffering from cardiovascular heart disease show clinically significant depressive and anxiety symptoms.
These symptoms can develop as a reaction to the illness or can be related to the direct effects of the drug therapies.
Sometimes, it becomes difficult to discriminate between both the illnesses but it is important to untangle them apart and treat both, as it might affect the prognosis of the problem and the treatment journey. The scientific guidelines suggest that pharmacological treatment combined with psychotherapy is the most effective strategy rather than sticking to any one modality of treatment.
Pharmacological treatment involves using medicines while psychotherapy popularly known as talk therapy entails using psychological means to treat problems that are emotional in nature.
According to Wolberg (1967), psychotherapy is a treatment in which a trained person deliberately establishes a professional relationship with the patient with the objective of
- Removing, modifying or retarding existing symptoms
- Mediating disturbed patterns of behavior and
- Promoting positive personality growth and development.
Three commonly used psychotherapeutic interventions for depression and anxiety are cognitive behavioral therapy (CBT), interpersonal therapy, and supportive therapy.
Cognitive Behavioural Therapy
According to cognitive behavioural therapy, depression and anxiety are cognitive disorders. They result from maladaptive cognitions or thinking patterns which in turn affect behaviour and emotions.
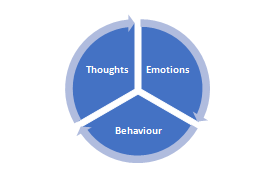
| CBT changes our emotional state by working on our thoughts and behaviors that are contributing to the distressing emotions. |
Imagine a professor crossing you in the hallway, you wish him good morning and that professor does not wish you back. If you were to have a thought of “he doesn’t like me,” it is likely to impact your emotional state and cause you to feel upset/anxious and to behave in an avoidant manner when you see him next.
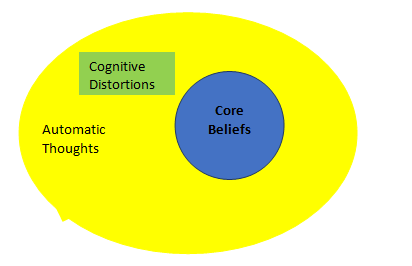
These are automatic thoughts that are dysfunctional, exaggerated, distorted, mistaken, or unrealistic which play a significant role in depression.
Let us look at this:
‘’Yes, I got second highest in maths, but it wasn’t a big deal and I still feel like a failure’’.
‘’ Rose got bad grades. Her mother believes it is because she is not a good enough parent’’.
These are examples of irrational or negative thinking in which the individual is either minimising their achievement or personalising an event which is not in their control. They are called cognitive distortions that are likely to make an individual susceptible to depression.
Also, every individual has core beliefs about self and the world. They are rigid and shape our overall perception and interpretation of the world. Sometimes they are not very helpful. For example: ‘’People are untrustworthy”
CBT involves cognitive and behavioral strategies which aims to identify and modify these irrational thinking patterns and maladaptive behaviors such as avoidance. It is highly structured and consist of 16 to 20 sessions. It requires a collaborative approach in which both the patient and the therapist work together to establish common goals in treatment which has been found to be one of the primary change agents in cognitive-behavioral therapy (CBT).
Interpersonal Therapy
In contrast to CBT, interpersonal therapy assumes that disturbing life events and interpersonal difficulties precipitate the symptom of anxiety or depression. It emphasizes on the role of cultural, social or familial values in the development of symptoms.
The four specific areas of emphasis include death of a loved one (grief), struggle with a significant other (interpersonal dispute), or some other life upheaval: a geographic or career move, the beginning or ending of a marriage or other relationship, or becoming physically ill (a role transition), or social isolation (interpersonal deficits).
It is a time-limited (acutely, 12-16 weeks) treatment with three phases: beginning, middle, and end.
The initial phase focuses on identifying the symptoms and link the target diagnosis to the interpersonal context in which it presents.
The middle phase of treatment deals with any of the four areas which requires intervention. This might involve helping the patient to mourn the death of a loved one or assume a new one in a role transition etc.
The last few sessions focus on termination, helping the patient feel more capable and independent by reviewing his or her accomplishments during the treatment.
Overall, the focus of the therapy is to modify the dysfunctional interpersonal relationships, resolve the disturbing life events, and eventually help patients build adequate social skills to organize their life.
Supportive Therapy
Supportive therapy is typically an unstructured therapy that relies on the basic ingredients of psychotherapy, such as reflection, empathic listening, education and encouragement. It is also called nondirective supportive therapy as the number of sessions and time are not defined. It does not require any active therapeutic strategy other than active listening and offering support. It focuses more on presenting problems rather than long-term difficulties. The overall goal is to reduce patients’ distress, provide psychological support and help them cope with their current circumstances.
There are a lot of other therapies as well which focus on depressive and anxiety symptoms. Please check with your therapist as to which one would suit you the best according to your profile and needs.
After this detailed description about different types of psychotherapies, the next question that pops in our head is, well, which one is the most effective therapy?
All of these therapies are backed up by strong scientific research for their efficacy. It is unwise to say that one of them is more effective than the other. The effectiveness of any therapy is determined by an individual and the presenting context. But the ultimate goal of each of these therapies is the same as Karen Horney says “to restore the individual to himself, to help him regain his spontaneity and find his centre of gravity in himself.”
Wishing you the best of mental health today and always!
HUDA NAAZ